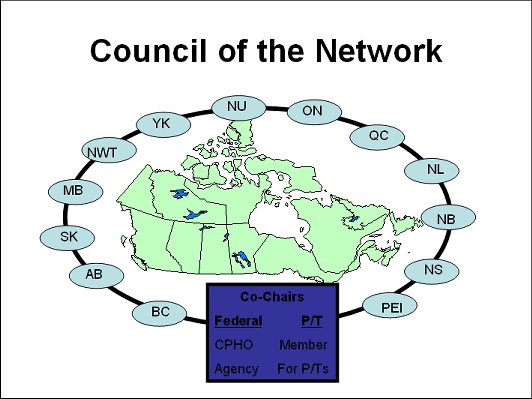
Members of the Council will facilitate the activities of the various parts of the Network. The Council will serve as a central governance body and will represent the Network to the public. The Council will serve as the senior body responsible for taking a strategic, coordinated view of the ongoing conduct and operation of the Network. It will be responsible for the instruments and tools of the Network and report annually to the Conference of Deputy Ministers of Health.
Membership of the Council will consist of one senior representative from each participating jurisdiction. In selecting their member, jurisdictions may wish to consider officials with decision-making authority who exercise leadership in a public health organization within government. While each jurisdiction is free to name whomever they wish to the Council, Deputies may wish to be guided by the fact that the role of the Council is to serve the policy and program needs of the CDM.
Council will be co-chaired by its federal and a P/T member to rotate among provinces and territories. Health Canada has indicated that the federal representative will be Dr. David Butler-Jones, Chief Public Health Officer (CPHO) of the Public Health Agency of Canada (PHAC). This should enable the Network to take advantage of the Agency as a focal point among several FPT groups of the Network.

- The key recommendation of our report is the creation of a Pan-Canadian Public Health Network, to be led by a Council of representatives of each jurisdiction (that I describe in the previous slide).
- Functionally, the Network, through the Council, gets its mandate from and is accountable to the Conference of Deputy Ministers of Health. It will report on an annual, and an as needed basis during public health emergencies. The Council provides leadership and oversees the day-to-day business of the Network.
- The vast majority of the work of the Network will be executed through a series of Expert Groups and Issue Groups on various public health topics. The Task Force has recommended six initial Expert Groups.
- Some of these Expert Groups (e.g. EPR, Lab Network, Communicable Disease) already exist and will be integrated into the Network, building on existing expertise and collaborative efforts that are working well.
Mandate of the Network
- The Network will function as a mechanism for intergovernmental collaboration and coordination on public health issues
- As such, the Network will:
- Facilitate information sharing among all jurisdictions;
- Disseminate information regarding best-practices in public health;
- Support the public health challenges jurisdictions face during emergencies;
- Provide advice and regular reporting to CDM on public health matters and the activities of the Network;
- Collaborate on the day-to-day operations of public health;
- Respect jurisdictional responsibilities in public health;
- Be accountable to the CDM
At the June 17th meeting of the Conference of Deputy Ministers of Health, Deputies asked the Task Force to clarify the role and mandate of the Network. The Task Force spent much of the summer considering and carefully developing the mandate of the Network so as to respect each jurisdiction’s responsibilities while also enabling jurisdictions to collaborate and coordinate on public health matters, when it is necessary and appropriate.
The mandate for the Network is two-fold: first there is a functional capacity to promote and facilitate F/P/T collaboration on public health issues when needed, and second, to respond to direction from the Conference of Deputy Ministers of Health on any public health matter.
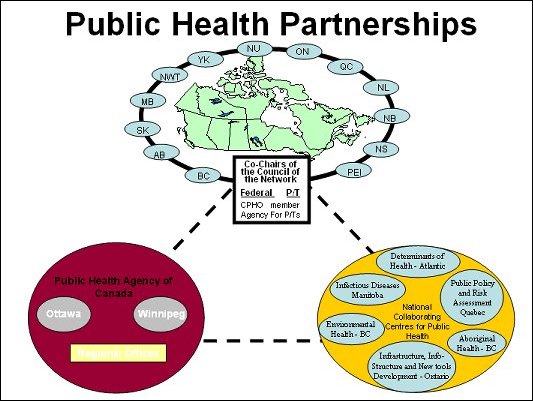
The Network will partner with other public health bodies, including the Public Health Agency of Canada and the six National Collaborating Centres for Public Health Science.
The six National Collaborating Centres for Public Health Science will establish linkages with public health experts in the regions, across jurisdictions and internationally. Within the PHN, the nature of these linkages will include association or affiliation across the various expert groups of the Network, to facilitate or support mutual public health activities of interest.
A properly structured and functioning public health system will contribute to:
- Improved levels of health status of the population and decreased health disparities
- Decreased burden on the personal health services system and thereby contribute to its sustainability
- Improved preparedness and response capacity for health emergencies
Mandate
- The Strengthening PH System Infrastructure Task Group was created with the following mandate:
To build on recommendations from the Naylor Report, as well as other pertinent reports, to address infrastructure gaps where F/P/T collaboration would be of benefit.

Analysis and Recommendations for Following Infrastructure Components:
- Sufficient & Competent Workforce
- Organizational Capacity
- Public Health Network and Expert Groups,
- Public health strategies and goals,
- Agreements and protocols,
- Public health legislation,
- Emergency response and surge capacity,
- Public communications and citizen engagement
- Information and Knowledge Systems
- Information, surveillance and infostructure
- Knowledge development and its translation into practice
- Cross-cutting Issues
- Public health laboratories
- Aboriginal health
- Collaborating centres for public health
- System resources
The Task Group ’s report outlines the many individual elements that comprise system infrastructure. While all require further development, there are some specific elements shown in the slide that were determined to be priorities and which were pursued in more detail in our report. These include elements for each of the three broad infrastructure categories, as well as a series of cross-cutting issues.
It is beyond the scope of this presentation to describe all of the recommendations for these priorities. Instead will highlight areas of recommendations for two areas: the public health workforce, and knowledge development and its translation into practice.
System Resources – Beyond Infrastructure
- Infrastructure is necessary, but insufficient for an effective public health system – strategies and programming
- Naylor estimates that about 2.6% of public sector health expenditures go to public health (about $2 billion/year)
- Estimates of required additional funding:
- UK’s Wanless Report, Costing of Quebec’s Public Health Program, BC’s Standing Committee and BC’s Cancer Society:
- Consistency in recommending a doubling of current expenditures with an increase to 5-6% of health expenditures.
Preceding slides have focused on our estimates of incremental investments in system infrastructure. Infrastructure supports effective programming and services, but does not include the costs of actually delivering those programs, which are much greater.
Doubling of the current investment in public health would provide an opportunity to fully implement the existing knowledge for effective practices and approaches. For example, if Canadian governments were to implement all nine effective program components for tobacco control that were identified by the U.S. CDC, it would cost $450 a year. Current federal spending on tobacco control is about $70M with additional spending by P/Ts. Clearly tobacco is but one risk factor and there are many public health priorities requiring attention.
Doubling funding is not the same as simply doing more of the same. One would expect greater comprehensive and inter-sectoral strategies and programs with better data to inform on progress towards objectives and goals.


PHSA strategic direction:
Prevention, Promotion, Protection
Expand our role as “knowledge resource” for the province by creating the capacity to link and use health information to reduce the burden of disease associated with chronic disease and support policy development.
Collaborate with other Ministries, municipalities, the voluntary and private sector and the regional health authorities to promote active healthy living and healthy public policy for British Columbians.
Gradually increase our emphasis on prevention, promotion and protection.
Strategic Direction: PPP
- Surveillance: link & use data and information to reduce the burden of chronic disease (prevention and control). Registries and databases in PHSA, the MoH, and other agencies such as CIHI & STC linked for various purposes:
- Primary prevention – data on SES, health behaviours linked with utilization and outcomes data for planning purposes
- Injury prevention & control
- Cardiac/renal/diabetes (Hi5) – obesity, nutrition, physical activity, tobacco data linked to burden of disease, PCI/CABG outcomes, ACS care.
- Primary health care – supporting local population-based initiatives
- Secondary prevention –
- AMI care
- DM care/renal care
- Cancer screening
Collaboration with other agencies to promote active healthy living: development of knowledge products and knowledge translation processes in tobacco, healthy weights, nutrition and physical activity.
- Tobacco:
- Cessation
- Taxation/enforcement
- Second-hand smoke
- workplace wellness
- Healthy weights:
- Consumer trends
- Food security
- Built environment
- Healthy urban planning guidelines
- Workplace wellness
Other collaborations
- BC Population Health network
- BC Healthy Living Alliance
- Pan-Canadian Healthy Living Strategy
- Chronic Disease and Injury Prevention and Control Expert Group (PHAC)
- Canadian Population Health Initiative (CIHI)
- International projects – OECD, etc
Strategic Direction: System-wide improvements
Develop networks in collaboration with RHAs in order to integrate quality care, provide equitable access and offer consistent standards for specific populations:
- PHC projects
- Renal
- Obstetrics
- Women’s health
- Shared care projects
- Penticton, Quesnel, Fraser , PG, BCCDC
- PHC data supports

Core programs in public health (MoH)
- Surveillance
- Prevention
- Protection
- Promotion
- First year developments:
- Food safety (BCCDC)
- Food security (PPP)
- Healthy living: tobacco, healthy weights (PPP)
- Air quality (BCCDC)
- Dental health (CH)
- Water quality (BCCDC)
HA core programs requirements
- Evidence review
- Indicators and performance measures
- Benchmarks
- Gap analysis
- Performance implementation plan
- HA targets
- Public reporting on performance
- Inclusion in performance agreements
PHSA Public Health Activities
- Surveillance: infectious disease, chronic disease, injuries, patient safety (BCCDC, BCCA, Trauma Registry)
- Protection:
- ID control (BCCDC)
- Environmental health – water, food, air, sewage, toxic exposures (NCC@BCCDC)
- Patient safety (BCCDC, PPP)
- Disaster preparedness (BCCDC)
- Prevention:
- Chronic disease control (tobacco, obesity, nutrition, physical activity, drugs & alcohol, etc) (PPP)
- Cancer prevention & screening (BCCA)
- Injury prevention (CH)
- Prevention of birth defects (C&WH)
- Promotion: workplace wellness, others
Opportunities
- Public Health Agency for Canada – $300M public health infrastructure
- National & provincial health goals
- Provincial MoH core programs – $8m, 16M & 24M for public health infrastructure
- SFU/UBC Schools of Public & Population Health
- International health initiatives