Primary Care Reform: Implications for Public Health
Posted on June 6, 2006
Page 3
So: system redesign is needed
Every system is perfectly designed to deliver the results it gets ‘- Berwick
First Ministers(2000): “planned provision of comprehensive services to a defined population…(with) …multidisciplinary teams..(and)…emphasis on health promotion, disease and injury prevention, and chronic disease management ..(and)..24/7 access to essential services”
Chronic Disease Management
Good early success with IHI collaborative model : diabetes, CHF
Challenge – many patients present with clusters of chronic disease e.g. ‘frail elderly’, DM,CHF, renal failure & mental health problems or chronic mental illness, addiction and HIV/hepatitis.
Urgent need for real system re-design
Important New Concepts
PHC teams providing care for a defined population
System re-design: improved health of population
Partnerships – clinicians, community agencies
Communication, information, decision supports
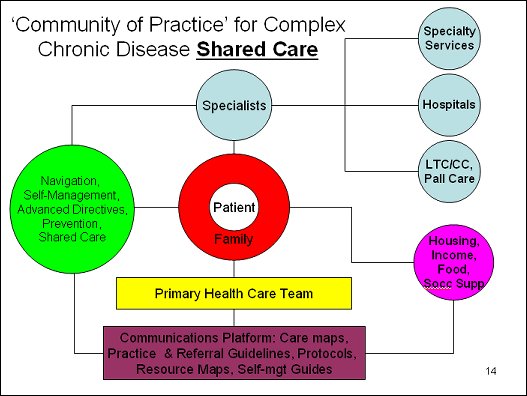
Shared care
Self-management/self efficacy
Navigation- care maps, resource maps
Better prevention
Evidence-based care- guidelines, protocols, algorithms, care pathways
Better information & decision supports
But what health system model?
Existing model – acute episodic care
Best available Canadian evidence – if focus is onimproving the health of a defined population then an ‘integrated community health model’ holds the most promise
Means an expanded primary care team integrated with hospitals, public health, home care, mental health, etc serving a defined (geographic) population
Achieved anywhere?
UK – PCTs & regional authorities
New Zealand – all personal (face-to-face) public health services delivered in primary care. PHO model.
Both countries achieved the transition to a new system through:
Vision – bottom-up & top-down
Organisation change management
Increased income for family docs
Significant investments in an EHR
Contents
This entry was posted in . Bookmark the permalink.